By the time you finish reading this blog, 71 newborns will have died globally, including 15 in India alone.
By the time you finish reading this blog, 71 newborns will have died globally, including 15 in India alone. Yet India has made major strides in reducing deaths of babies within the first 28 days of life. Recent reports suggest that more than eight in ten women deliver in health facilities, although COVID-19 has affected this. In a setting with a high institutional delivery rate, more of the newborns who need life-saving critical care are in healthcare settings instead of in the community. Special Newborn Care Units are available in over 80% of districts in the country, to treat small and sick newborns using a well-established care package which addresses the primary causes of deaths, including prematurity, complications at birth and sepsis. Despite the increased availability of services for women and newborns, there is an urgent need to ensure that the quality of care is improved.
Quality improvement collaboratives
Evidence shows that training of health care workers alone is not sufficient. Instead, quality improvement collaboratives may offer potential to improve the quality of health care services. Working as a team, health care professionals identify and prioritise an area for improvement, for example reducing mortality in the newborn care unit where they work. With support from a quality improvement mentor, the team introduce and test innovations in incremental steps through Plan-Do-Study-Act cycles. In quality improvement collaboratives, or learning collaboratives, teams from different facilities often come together in so-called ‘learning sessions’ to share ideas and lessons learned on what worked or didn’t work [1].
Safe Care Saving Lives
The Safe Care Saving Lives programme, implemented by ACCESS Health International, was one of the first quality improvement collaboratives to work in Special Newborn Care Units in Telangana and Andhra Pradesh, in Southern India. The programme aimed to reduce the number of newborn deaths by improving 20 evidence-based practices for delivery and newborn care, each known to save lives. These included kangaroo mother care, hand hygiene when handling the baby, and always taking a baby’s temperature at admission.
The Safe Care Saving Lives programme was also one of the few quality improvement collaboratives in maternal and newborn care to be rigorously evaluated, through a study conducted by the London School of Hygiene & Tropical Medicine and the Public Health Foundation of India. The evaluation compared changes from 2016 to 2018 in 29 hospitals receiving the intervention with 31 hospitals that did not. Although average numbers of newborn deaths reduced in the intervention hospitals, this also happened in the comparison hospitals (figure below). The study concluded that the programme had no impact on facility-based newborn deaths or stillbirths and did not change adherence to the 20 targeted evidence-based practices. But it did highlight three important lessons for future quality improvement initiatives [2].
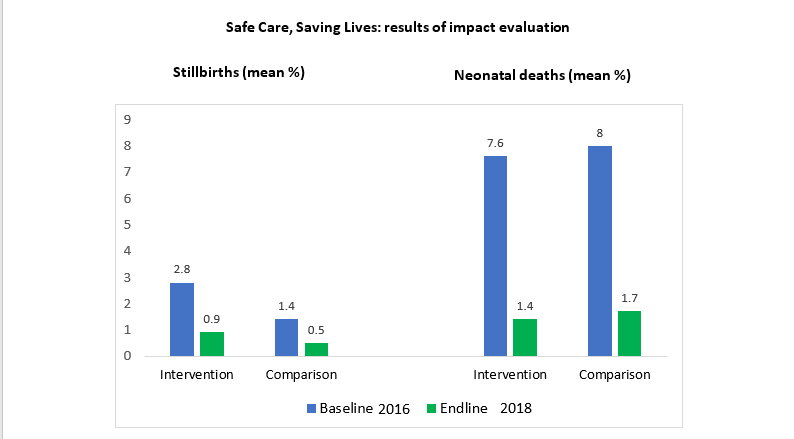
Between 2016 and 2018, the mean number of stillbirths went down in both intervention and comparison hospitals by very similar amounts (difference-in-differences -1%, 95% confidence interval -2 – 0.2). Similarly, mean neonatal deaths also reduced over time, by the same amount in both intervention and comparison hospitals (difference-in-differences 0%, 95% confidence interval -10, 10).
Three lessons for quality improvement initiatives
1. Bring hospital leaders onboard
Engaging the large private and public hospitals was a challenge. Of the 29 hospitals recruited into the programme, only seven remained engaged 16 months later.
Engaging hospital leaders is a key part of a quality improvement intervention. What motivates them? How can quality improvement be aligned to their priorities? Who are the quality champions that can be mobilised to gain and sustain their buy-in? And what specific strategies are needed to engage medical colleges, private hospitals and district hospitals? These emerge as important questions for the design of a future intervention.
In the words of one of the mentors working on the programme,
“Generally there will be a resistance because […] quality is not compulsion to any government hospital and it is their choice to implement it or not. If the leadership wants it strongly, then the staff obviously do it… but they do it forcibly. If the staff wants to develop their own unit, they do it.”
2. Focus on whole groups of evidence-based practices that address the biggest problem
Focusing on improving a few evidence-based practices was not sufficient. In Telangana and Andhra Pradesh, prematurity was the leading cause of newborn deaths [3], and the quality improvement package relating to prematurity included five evidence-based practices (Figure below). While several hospitals worked on improving kangaroo mother care, only one hospital focused on improving all five recommended practices. Some hospitals did not work on prematurity at all. First and foremost, quality improvement needs to be problem-driven, supported by local data to identify priorities.
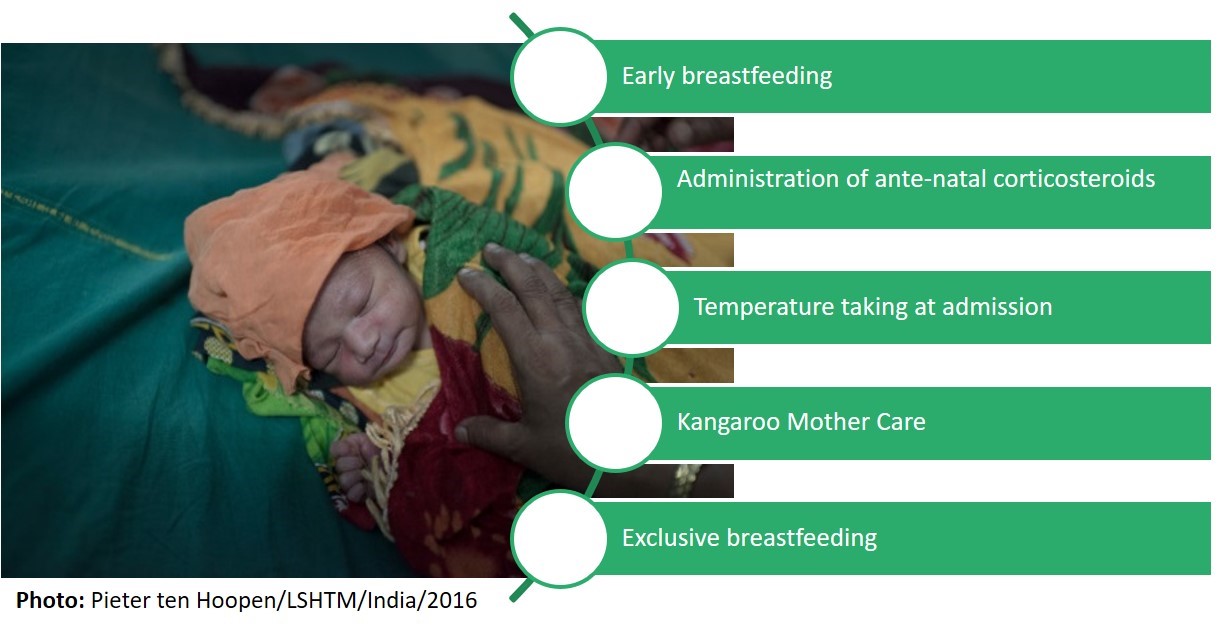
Evidence-based practices for prematurity addressed by Safe Care Saving Lives
3. Plan beyond individual facilities
The highest newborn mortality in Special Newborn Care Units is among babies referred from other settings. Often, referrals come from hospitals that have Newborn Care Units themselves [3]. The Safe Care Saving Lives programme initiated collaboratives linking Newborn Care Units in secondary hospitals with their tertiary referral centre for small and sick newborns. However, this only started in 2018.
When designing future quality improvement initiatives, implementers should ask themselves:
- ‘At which level should we implement this initiative to have the most impact on newborn mortality?’
For instance, a focus on referral clusters, rather than single health facilities, could yield better results.
- ‘Which institutions need to collaborate to enable a systems approach to quality improvement, and how can we facilitate a successful collaboration?’
There is strong potential in leveraging the leadership of professional associations and networks.
References
- Kilo CM. A framework for collaborative improvement: lessons from the Institute for Healthcare Improvement’s Breakthrough Series. Qual Manag Health Care. 1998;6(4):1-13.
- Zamboni K, Singh S, Tyagi M et al. Effect of collaborative quality improvement on stillbirths, neonatal mortality and newborn care practices in hospitals of Telangana and Andhra Pradesh, India: evidence from a quasi-experimental mixed-methods study. Implementation Science 16, 4 (2021). https://doi.org/10.1186/s13012-020-01058-z
- Hanson C, Singh S, Zamboni K, Tyagi M, Chamarty S, Shukla R, et al. Care practices and neonatal survival in 52 neonatal intensive care units in Telangana and Andhra Pradesh, India: A cross-sectional study. PLoS Med. 2019;16(7):e1002860. https://doi.org/10.1371/journal.pmed.1002860
Acknowledgements
The evaluation was funded by the Children’s Investment Fund Foundation.
